

Recent upticks in the rates of sexually transmitted infections continue to expose deep racial disparities in the American maternal health care system, from syphilis and HIV to gonorrhea.
It’s been well-documented that Black Americans are disproportionately affected by STIs. This is due in large part to systemic barriers to quality health care, such as having limited access to full health insurance coverage and comprehensive sex education — particularly in more conservative Southern states, where over half of the country’s Black population resides.
Read more: STD Rates Are on the Rise. Are Black Communities More Open To Talking About Them?
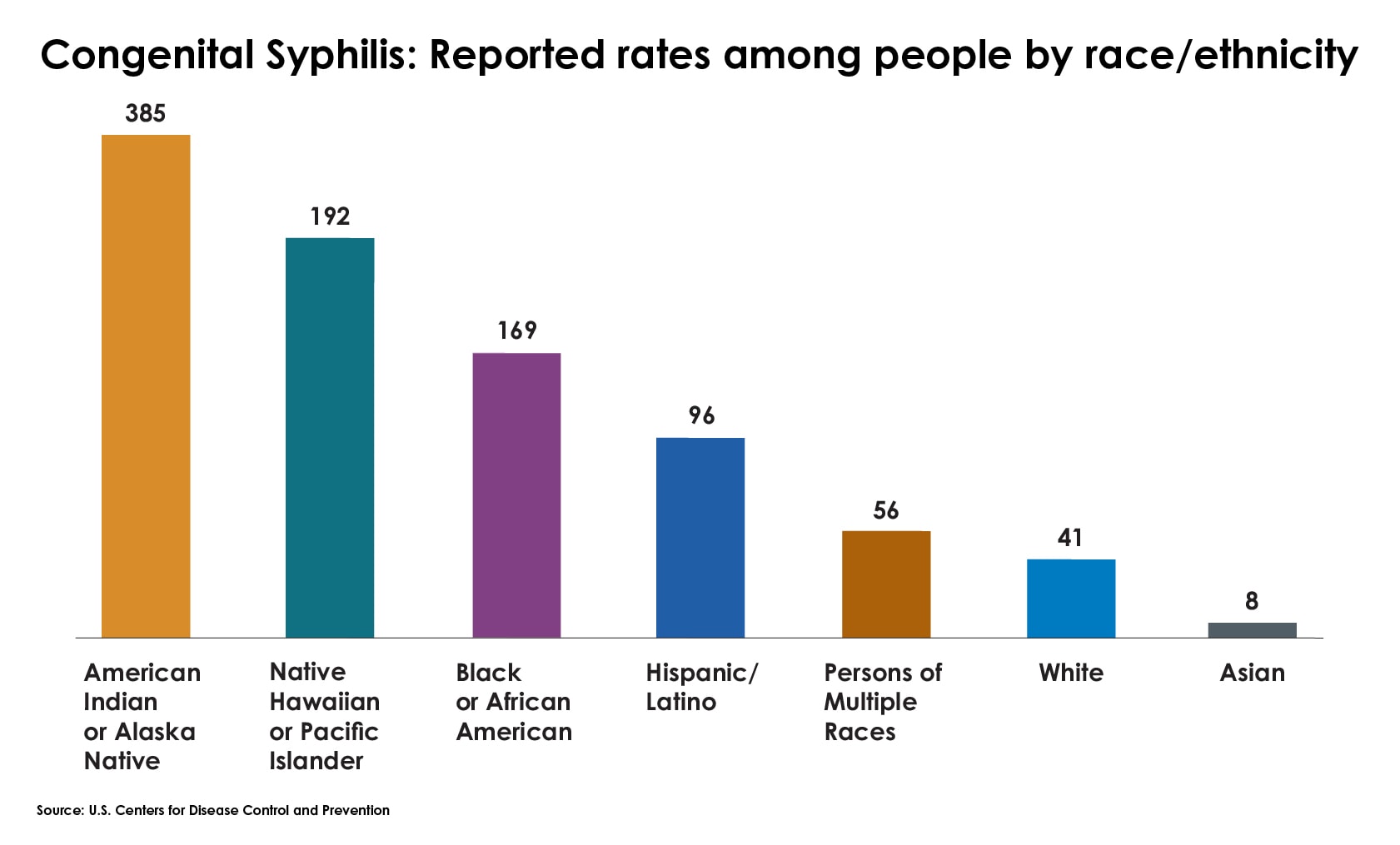
Data shows that infants born to Black or Hispanic mothers are up to four times more likely to contract congenital syphilis, according to the Centers for Disease Control and Prevention, which can lead to complications for both the mom and baby. It’s a disease that’s efficiently managed with antibiotics, but prescription shortages and difficulties accessing care pose a barrier for some Black patients.
{kind=link}
Across the U.S., the number of such cases reported among newborns ballooned from 335 in 2012 to over 3,700 in 2022. That’s more than 10 times the number of cases over the course of the decade, and it resulted in 231 stillbirths and 51 infant deaths last year, in what one official called “an unacceptable American crisis.”
Here’s what you need to know, according to Dr. Yolanda Lawson, a Texas-based OB-GYN and president of the National Medical Association. The conversation has been condensed and lightly edited for clarity:
Where are we right now in terms of STI rates in the Black community? What should folks know?
Yolanda Lawson: When I went to medical school, we were taught that syphilis was eradicated. While there’s no vaccine for it, we knew how to treat it. We were taught in such a manner that I really didn’t think I would see syphilis. Now, it is common for me to have to treat individuals with it. School, for me, was in the late ’90s. I finished in 2002.
We know that Blacks and Hispanics have a higher rate for syphilis. There’s also higher rates for congenital syphilis among Hispanic and Black babies. For them, we know it can be a leading cause of blindness, and other musculoskeletal or lifelong disabilities. It’s quite important to make sure that pregnant women understand the importance of testing. The problem with syphilis is it can live dormant in your system.
What should folks know about testing and how to protect themselves given the disparities?
We absolutely saw increased rates during and after the pandemic. We saw increased rates of depression, which led to increased rates of perhaps recreational drug use and alcohol use as well as loneliness, which can impact things like condom use. We were supposed to be distancing socially, but there were other psychological and emotional impacts, whether it was grief, or what have you.
The other issue was the delay in diagnosis. Because people may not have been coming in, we implemented a lot of remote testing, but at-home kits were complicated. People aren’t thinking about STIs. I have same-sex couples, especially with women, who may not think they’re susceptible because they’re not with a man, which is not true.
When you go for STI testing, we need to make sure that all patients are getting comprehensive tests and that it’s not only gonorrhea and chlamydia. It’s very important that people know what they’re getting tested for. Some providers may not even do an HIV test.
With syphilis rates, in particular, skyrocketing, what do we know about treatment?
The preferred treatment is an injection. It’s a single dose, if we know how long you had it. A problem I have is that sometimes people don’t know how long they’ve had it. Then, that requires three injections.
But when you start thinking about the social determinants of health, we have to go through a lot to get people to come back, complete therapy, retest to make sure everything is OK. Getting folks in can be a barrier. A lot of times, I may diagnose you and have to send you to the health department. They can’t just go to the pharmacy and pick up a pill.
I’m in Dallas. I’m downtown. I’m not in rural America, and I even have challenges getting my patients treated.